Summary
- Autism is defined behaviourally, and classified as neurodevelopmental disorder
- Autism rates are increasing, and technical changes to definitions, diagnosis, or awareness cannot fully explain the increase
- Genetics plays a role, but there must be environmental factors that cause autism, and there may be multiple factors
- Aluminum is a neurotoxin that can have subtle neurological effects
- Aluminum from infant vaccines exceeds the WHO safety level
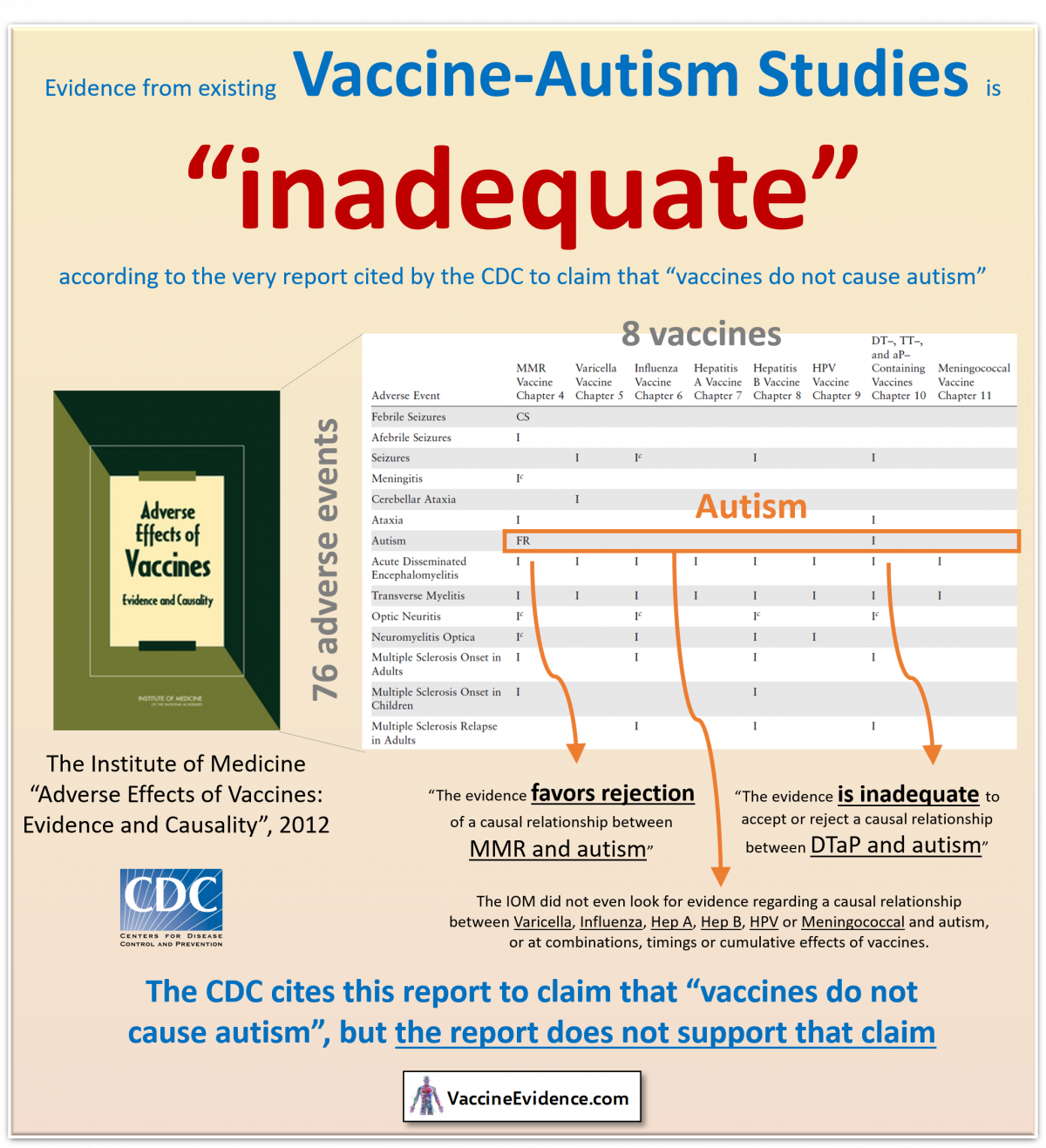
- No large-scale epidemiological studies have been carried out looking for an association between aluminum-containing vaccines and autism.
- Several small-scale epidemiological studies found an association.
Autism is neurological
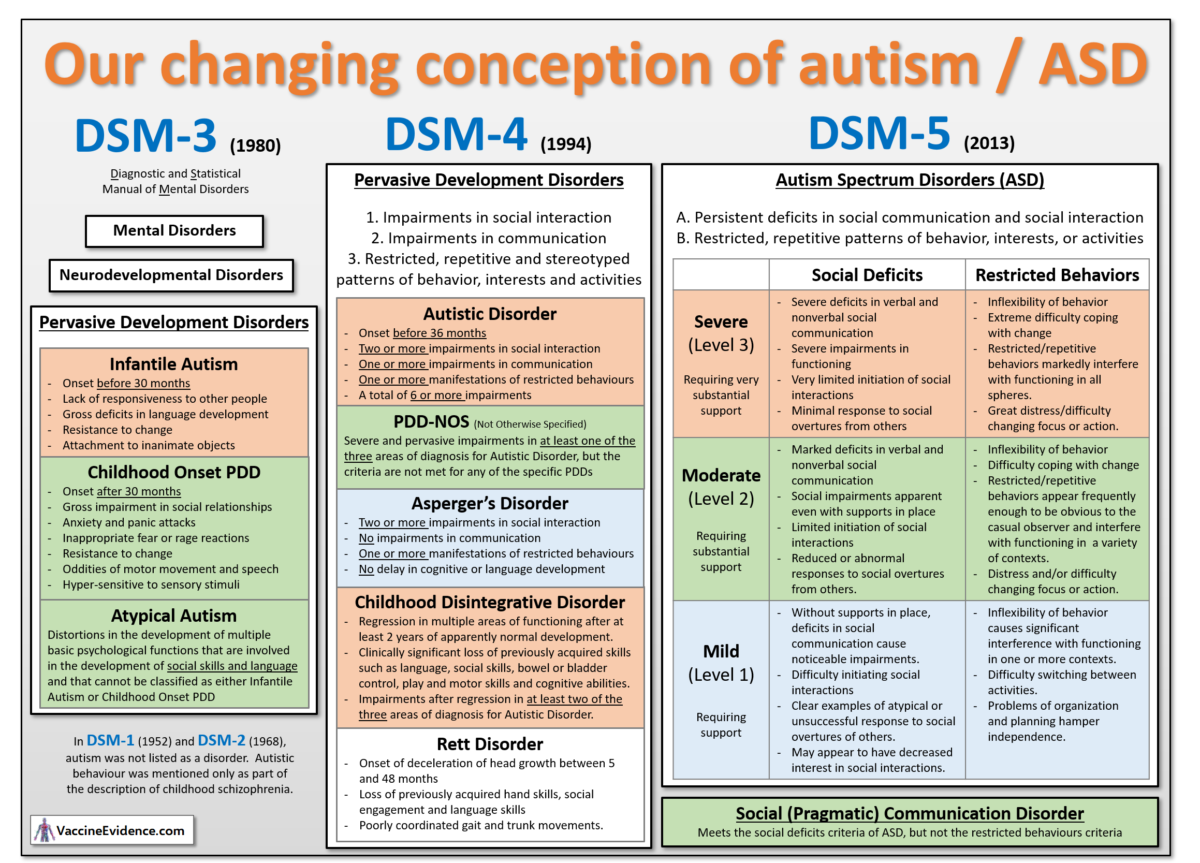
Autism is defined behaviourally by the two characteristics: 1) Persistent deficits in social communication and social interaction across multiple contexts, and 2) Restricted, repetitive patterns of behavior, interests, or activities. This definition comes from DSM-5 (2013), which classifies autism as a neurodevelopmental disorder, a type of mental disorder. There are three levels of severity on each characteristic, based on the extent of support required.
Something is causing children’s brains to be altered during neurodevelopment, resulting in autistic behaviours. Shouldn’t we try and find out what is causing that? An investigation into cause does not require any judgement about whether more autistic children is “good” or “bad”, or whether being autistic is a strength or a weakness. It is merely an attempt to explain the observation that autism occurs and is increasing.
The autism rise is real
The number of people diagnosed with autism has increased dramatically since 1985, from 1-in-10000 to 1-in-35, and the number is still increasing rapidly (Nevison, 2014). This dramatic rise cannot be explained by changes to the definition of autism or to improved diagnosis and awareness. Something is causing more children to develop autism. The increase is real, not technical (Nevison, 2017).
Autism has an environmental cause
The increase is too rapid to be explained as genetic, so the cause must be environmental. We know from twin studies that autism is partly genetic and partly caused by environmental factors (Hallmayer, 2011).
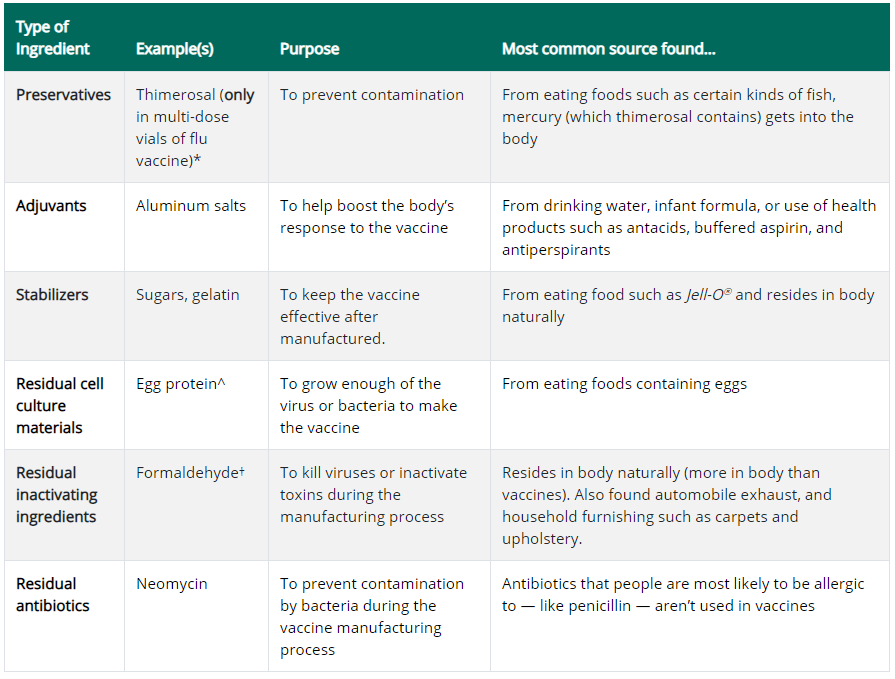
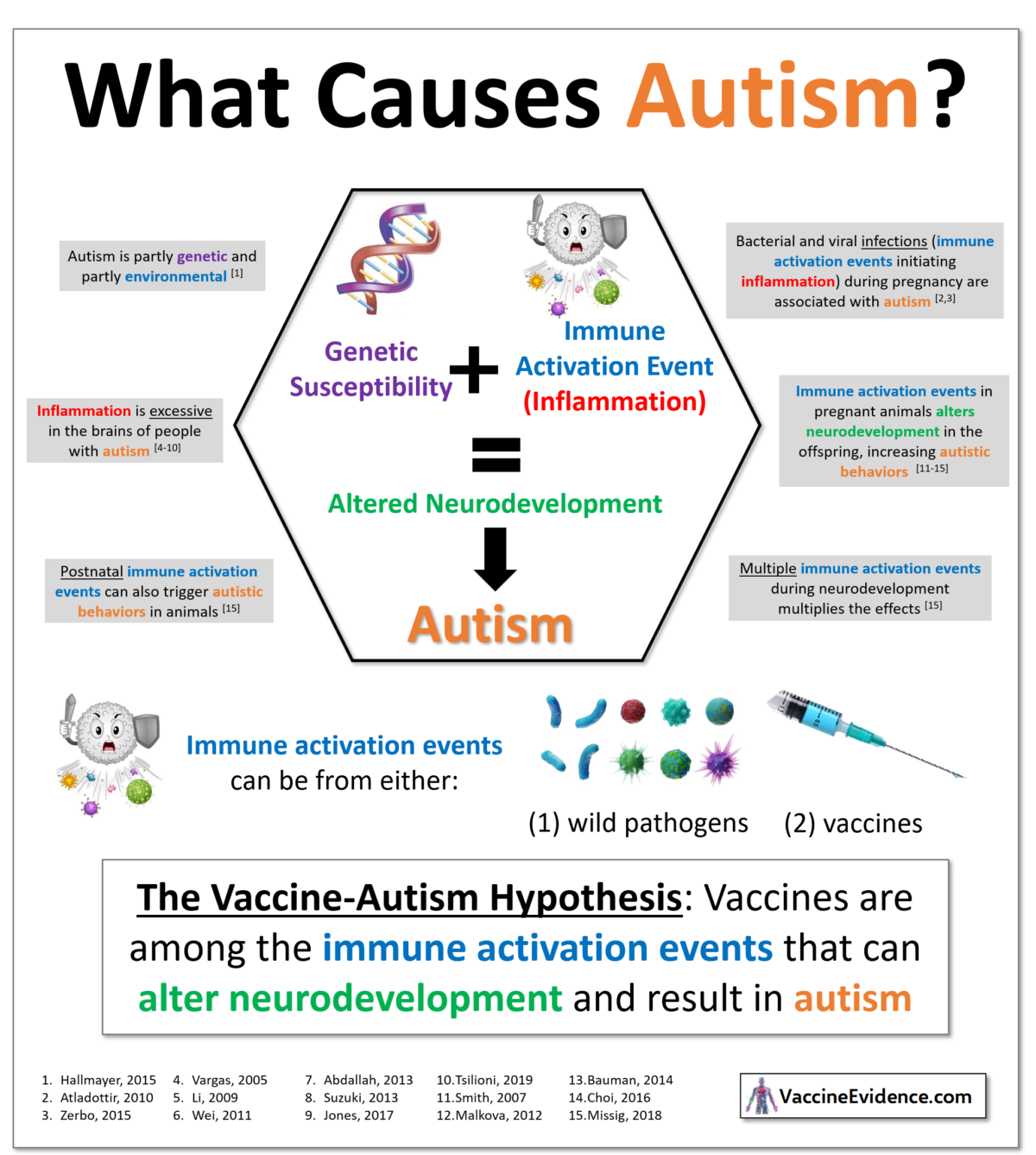
Autism has been linked to multiple environmental toxins, including glyphosate, electro-magnetic frequencies, and vaccine ingredients such as aluminum and thimerasol (Mercola, 2018). Environmental toxins activate the innate immune system and initiate the inflammatory process. Inflammation is excessive in the brains of autistic people, demonstrating neurotoxicity (Vargas, 2005 and Tsilioni, 2019).
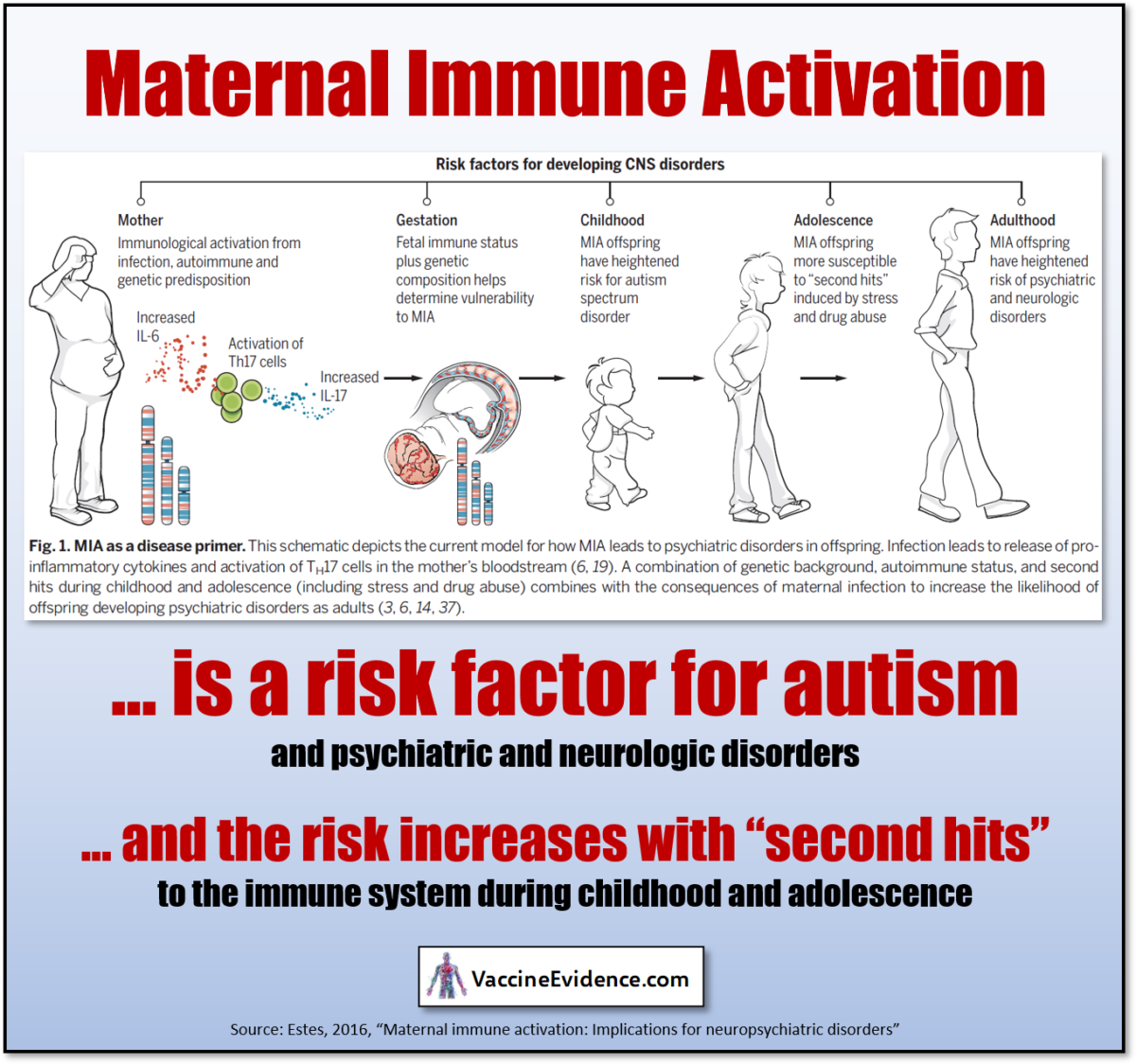
Maternal immune activation (MIA) has been identified as a cause of autism, through both epidemiological and animal studies. A severe infection during pregnancy is associated with autism (Zerbo, 2015). Autistic behaviours can be induced in animals by activating the immune system during pregnancy (Malkova, 2012). Post-natal immune activation has also been found to cause autistic behaviours in animals (Missig, 2018).
The particular toxin or pathogen appears to be less important than the strength and timing of the immune activation during early neurodevelopment. This is why any or all of the above-mentioned environmental toxins could be a cause of autism. Since the focus of this website is vaccines in general, and aluminum toxicity in particular, I will explain specifically why aluminum in vaccines is a likely cause of autism.
Aluminum is a neurotoxin that can have subtle neurological effects
Aluminum toxicity has been recognised as a major cause of encephalopathy (brain damage) in uremic patients, whose kidneys are less effective at eliminating aluminum (Alfrey, 1993).
Aluminum can have more subtle neurological effects, only detected through behavioural tests, even when the kidneys are healthy. Subtle neurological effects have been observed in workers chronically exposed to aluminum dust or fumes (ATSDR, 2008). Preterm babies exposed to high levels of aluminum through Total Parenteral Nutrition (TPN) scored lower in mental development tests (Bishop 1997), leading the FDA to place a limit on aluminum content in TPN products (FDA, 21CFR201.323).
In animal models, aluminum at sufficient doses in the diet induces: neuroinflammation (Viezeliene, 2013); loss of neuronal dendritic spine and cognition impairment (Cao, 2016); memory impairment (Martinez, 2017); adverse reproductive effects (Hirata-Koizumi, 2011); learning delay (Bilkei-Gorzo, 1993); decreased limb strength (Poirier, 2011); and decreased motor performance (Golub, 2001).
Based on these animal studies, health agencies such as the WHO (JECFA, 2011) have established safety limits for oral intake of aluminum. The current WHO oral intake safety limit is 0.3 mg/kgbw/day.
High levels of aluminum have been observed in the brains of individuals who had neurological conditions, including Alzheimer’s disease (Mirza, 2017) and autism (Mold, 2018). A meta-analysis showed that excessive aluminum in blood, urine, and hair is associated with autism (Sulaiman, 2020).
Given all this, we ought to be deeply concerned with the possibility that aluminum toxicity may be altering the neurodevelopment of children, resulting in autism.
Aluminum from infant vaccines exceeds the WHO safety level
The primary source of exposure to aluminum during infancy is from vaccines. Exposure through diet and air is limited by very low permeability of the gut and lung linings to aluminum. The aluminum in vaccines on the other hand all enters systemic circulation, since it has no other way of leaving the injection site. Over the whole of infancy, uptake of aluminum from vaccines is around 50x higher than uptake from breast milk and air, as I demonstrated here.
The WHO oral intake safety level of 0.3 mg/kgbw/day can be converted into an uptake safety level by multiplying the oral intake safety level by the gut bioavailability of ingested aluminum. When this is done, it can be seen that aluminum uptake from vaccines exceeds the implied WHO uptake safety level, as I demonstrated here.
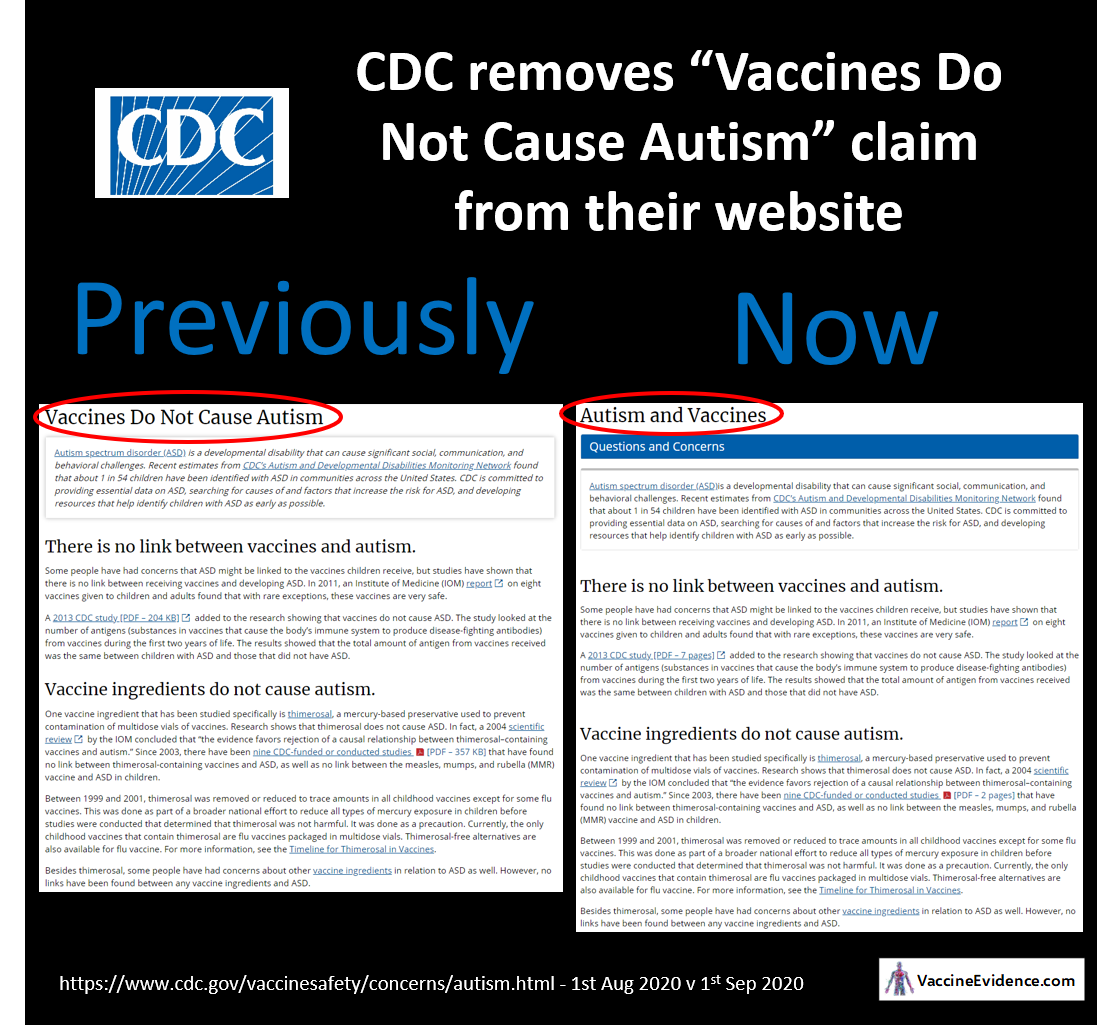
The only evidence cited by the CDC that the amount of aluminum in infant vaccines is safe is a pharmacokinetic model (Mitkus, 2011) which has many critical errors and weaknesses; I wrote about one of them here.
No large-scale epidemiological studies
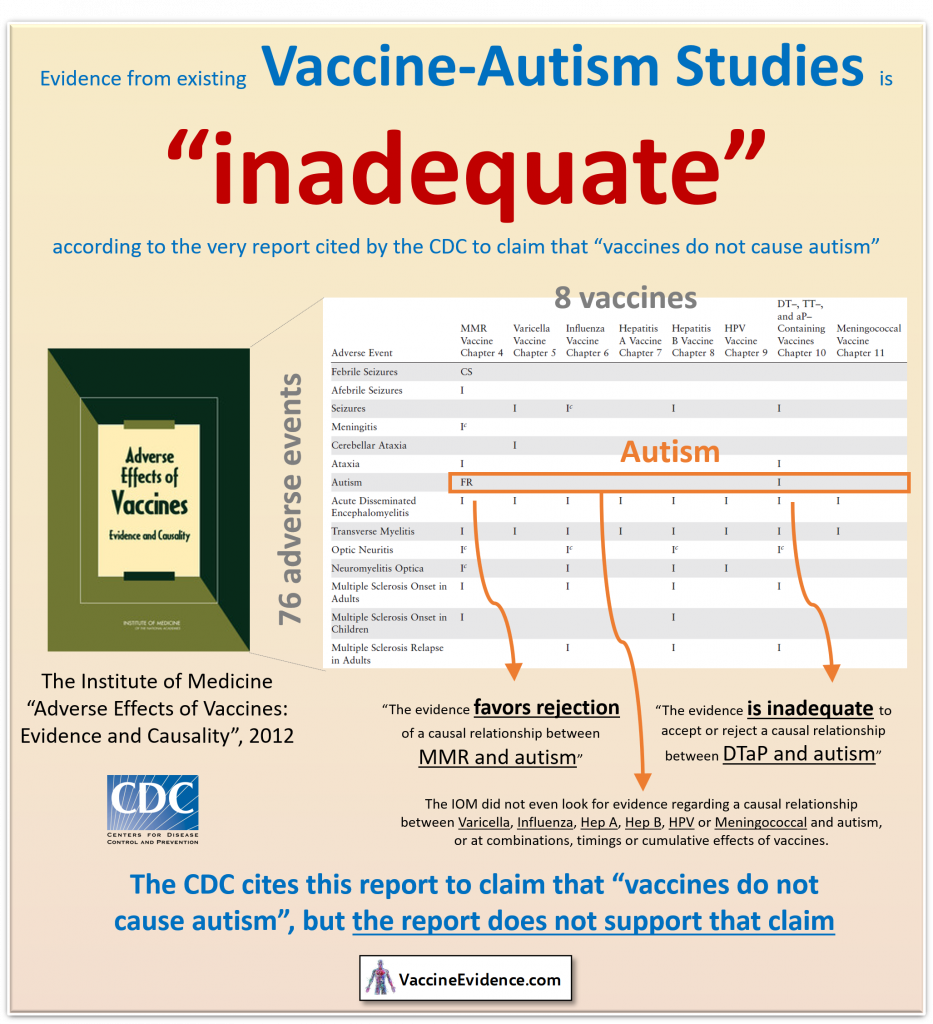
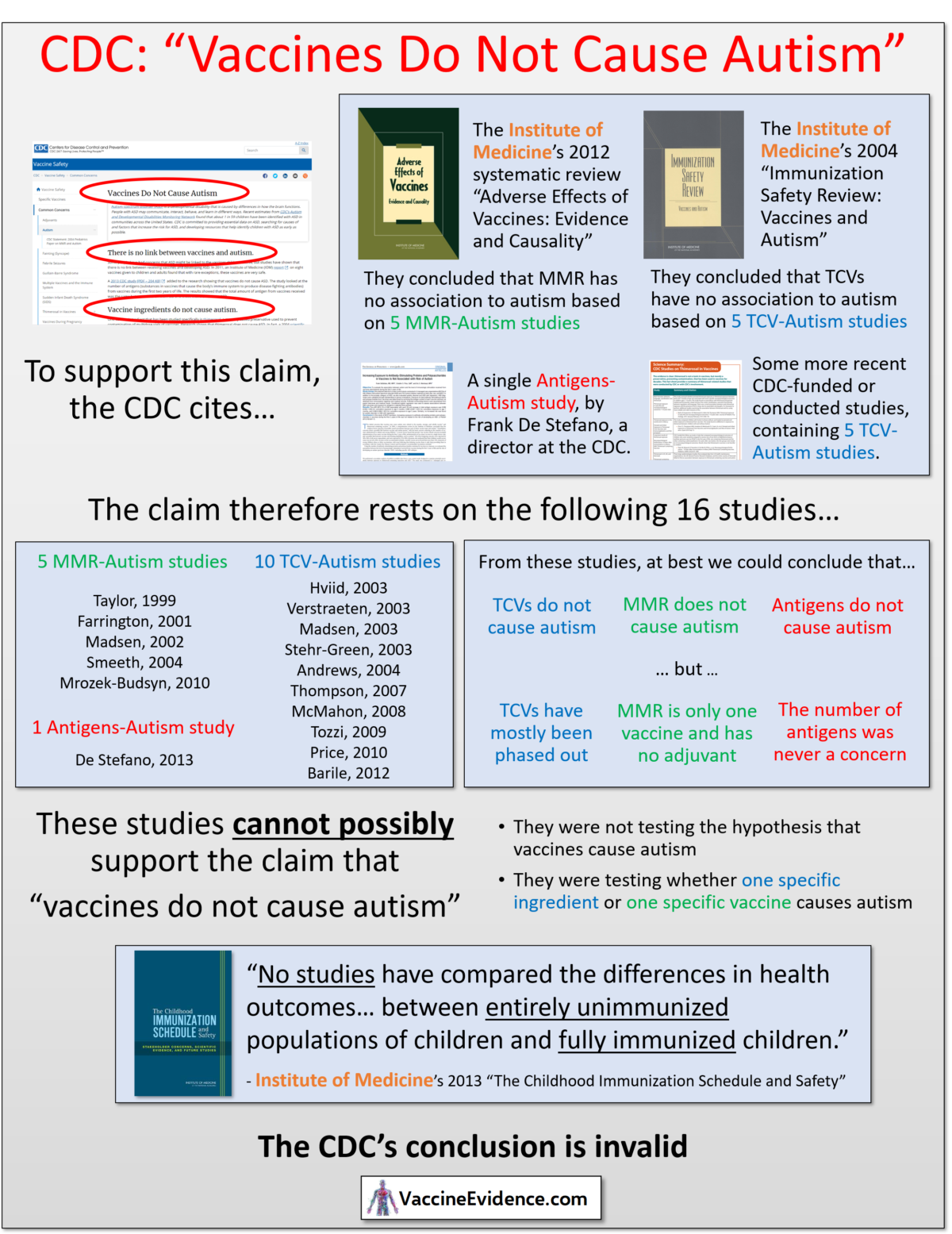
No large-scale epidemiological studies have been carried out looking for an association between aluminum-containing vaccines and autism (IOM, 2012). The vaccine schedule as a whole has not been tested (IOM, 2013)
This is despite the existence of an extensive database called the Vaccine Safety Datalink (VSD), controlled by the CDC. The Institute of Medicine described the VSD as the most feasible way to conduct large scale-studies comparing health outcomes of vaccinated and unvaccinated children (IOM, 2013), but still no such studies have been done.
Small-scale epidemiological studies found an association
Some independently-funded small-scale epidemiological studies have been conducted:
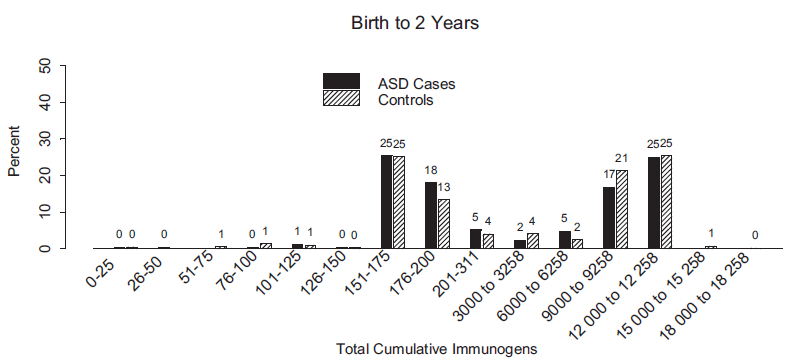
- an ecological study that found that autism rates are higher in countries with schedules where aluminum-containing vaccines are given earlier, and that 8 of 9 of Hill’s criteria for establishing causality are satisfied in the case of aluminum and autism (Tomljenovic, 2011)
- a pair of cross-sectional studies that found an association between the aluminum-containing Hepatitis B vaccine and developmental disability and autism (Gallagher, 2008 and Gallagher, 2010)
- a survey of parents of 666 homeschooled children that found an association between vaccinations and neurodevelopmental disorders, allergies, and eczema (Mawson, 2017)
- a retrospective cohort study of 2,047 children across three paediatric practices found an association between vaccines and developmental delay, ear infections, and asthma (Hooker, 2020).
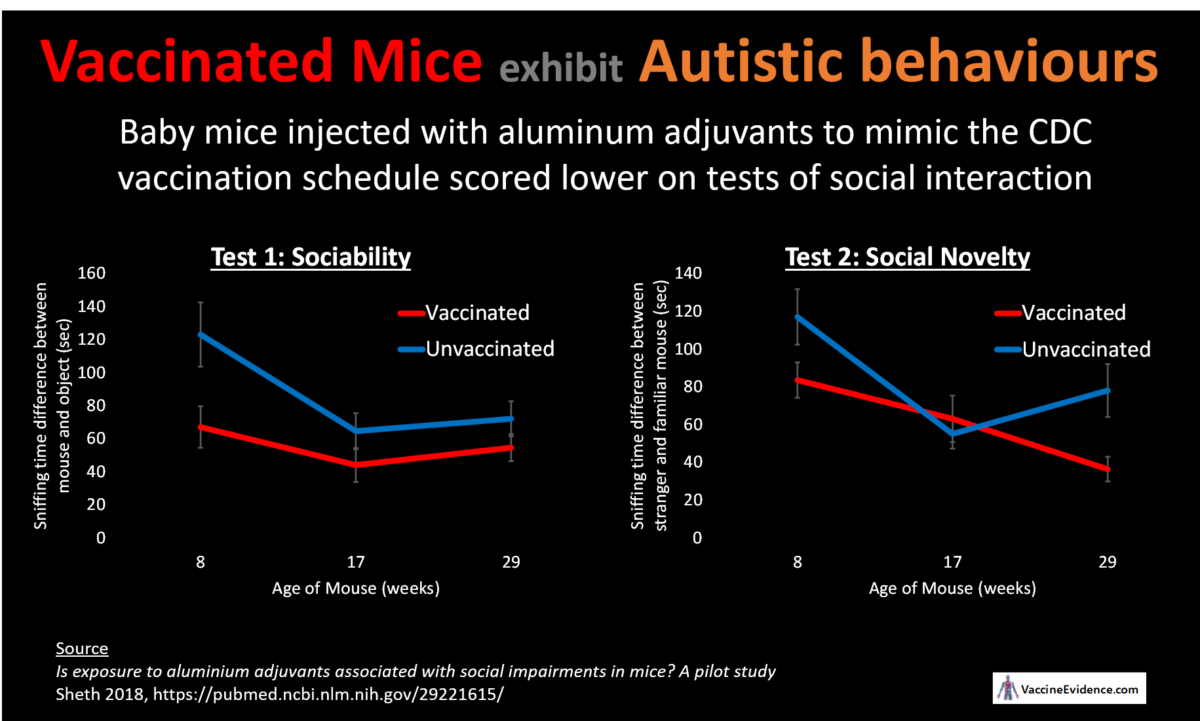
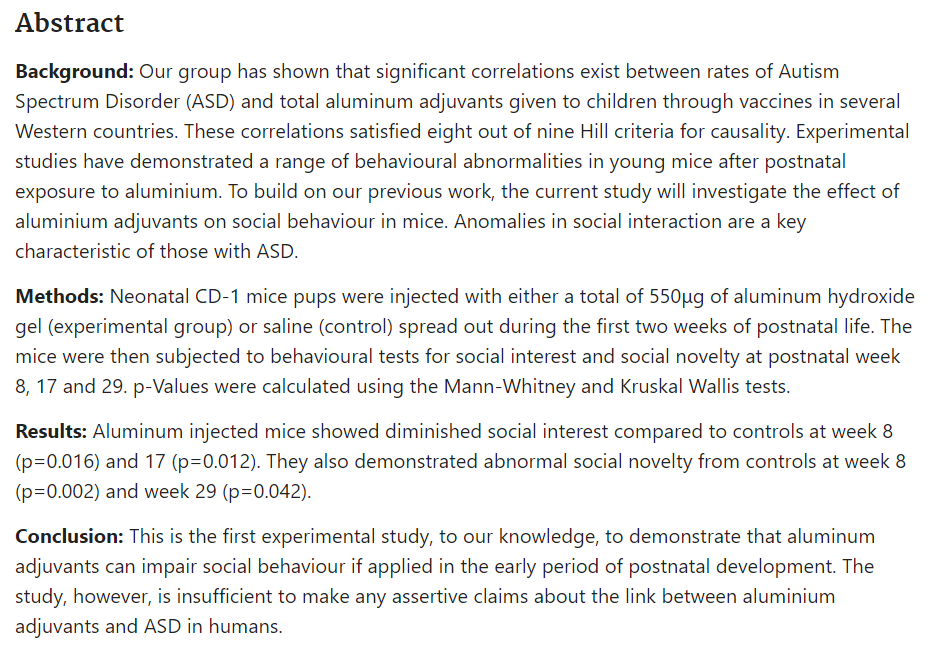
Finally, mice vaccinated to mimic the CDC recommended schedule were found to exhibit autistic behaviour (Sheth, 2018).
Conclusion
Given this abundance of evidence implicating aluminum in vaccines as a likely cause of autism, it is urgent that large-scale epidemiological studies are carried out to test this highly-plausible hypothesis. Parents need to be informed about the evidence that the aluminum in vaccines can alter the neurodevelopment of their children.