This post is my review of the CDC webpage titled Adjuvants and Vaccines.
What is an adjuvant?
The CDC writes:
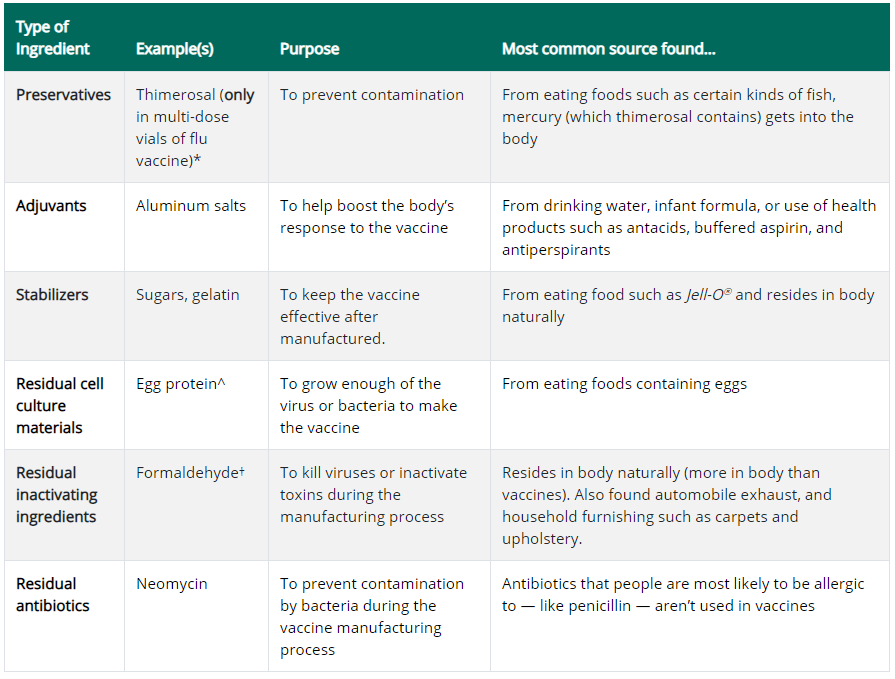
An adjuvant is an ingredient used in some vaccines that helps create a stronger immune response in people receiving the vaccine. In other words, adjuvants help vaccines work better. Some vaccines that are made from weakened or killed germs contain naturally occurring adjuvants and help the body produce a strong protective immune response. However, most vaccines developed today include just small components of germs, such as their proteins, rather than the entire virus or bacteria. Adjuvants help the body to produce an immune response strong enough to protect the person from the disease he or she is being vaccinated against. Adjuvanted vaccines can cause more local reactions (such as redness, swelling, and pain at the injection site) and more systemic reactions (such as fever, chills and body aches) than non-adjuvanted vaccines.
By design then, vaccine adjuvants are necessarily toxic. This is because their purpose is to induce an immune response stronger than the immune response to the antigen component alone. The adjuvant is what makes the challenge to the immune system from the vaccine strong enough to induce immunological memory.
This is why the safety of vaccine adjuvants is so important to the safety of vaccines as a whole; the adjuvant is by design the most toxic part of the vaccine.
Aluminum Salts
The CDC writes that:
Aluminum salts, such as aluminum hydroxide, aluminum phosphate, and aluminum potassium sulfate have been used safely in vaccines for more than 70 years. Aluminum salts were initially used in the 1930s, 1940s, and 1950s with diphtheria and tetanus vaccines after it was found they strengthened the body’s immune response to these vaccines.
Aluminum salts have indeed been used since the 1930s, as described in the earliest papers about aluminum adjuvants, such as Glenny 1926 and Volk 1942. Whether they have been used safely is the question at hand.
There were no safety studies done on the effects of Aluminum-Containing Vaccines (ACVs) prior to their routine use in infants. The only studies were of efficacy, tested by measuring antibodies. The first routine ACVs were the diphtheria, tetanus, and pertussis vaccines. These were later given as a combined vaccine, known as DTP, and then DTaP (the ‘a’ referring to acellular pertussis).
Up until 1990, the DTP vaccine was the only ACV given routinely to infants. After 1990 however, the number of ACVs on the recommended infant vaccine schedule started increasing. The Hib and Hepatitis B vaccines were added in 1991 and the Pneumococcal vaccine in 2000. They started being given in more doses and at a younger age. Infants today are considerably more exposed to aluminum from vaccines than infants of 30 years ago.
Aluminum and Neurodevelopmental Disorders
Aluminum is classified by the US Agency for Toxic Substances and Disease Registry (ATSDR) as a neurotoxin. This means the first harmful effects of aluminum overdose occur in the brain. The ATSDR describe aluminum as having “subtle neurological effects”, even at low doses. A steady increase in neurodevelopmental disorders, e.g. ASD, ADHD, and intellectual disability, is to be expected if aluminum adjuvants in infant vaccines are altering neurodevelopment.
We have seen an increase in neurodevelopmental disorders in line with increasing exposure to aluminum from vaccines. The increase cannot be explained away as expanded definitions, better diagnosis, or increased awareness. This ecological observation – the temporal correlation between ACV use and neurological disorders – calls for further research. As a neurotoxin, aluminum has to be a prime suspect in the search for causes of neurodevelopmental disorders.
Newer Adjuvants
The CDC writes that:
Newer adjuvants have been developed to target specific components of the body’s immune response, so that protection against disease is stronger and lasts longer.
None of the newer adjuvants are yet used in infant or childhood vaccines. They are thus of no relevance to an investigation of adjuvant safety in the infant and childhood vaccine schedule. The safety of adjuvants in this context means the safety of aluminum salts.
Safety Testing – Clinical Trials
The CDC writes that:
In all cases, vaccines containing adjuvants are tested for safety and effectiveness in clinical trials before they are licensed for use in the United States, and they are continuously monitored by CDC and FDA once they are approved.
In pre-approval clinical trials, potential new vaccines are tested against a placebo injection. The primary focus of the trials is efficacy; a vaccine is judged as successful when it results in the development of antibodies. Safety is a secondary consideration. Typically, immediate adverse reactions are recorded, there is active follow-up for only a week, and passive follow-up for only a year.
Pre-approval clinical trials will not pick up long-term adverse reactions, chronic conditions or altered neurodevelopment. No rare adverse events are picked up in the clinical trials, due to the small sample size.
For assessing adjuvant safety, pre-approval clinical trials are entirely useless. This is because both the vaccine being tested and the placebo contain adjuvant! The placebo is either a solution of adjuvant only, or an already-licensed vaccine. There are no safety tests of vaccine adjuvants in pre-approval clinical trials of ACVs.
Safety Testing – Monitoring
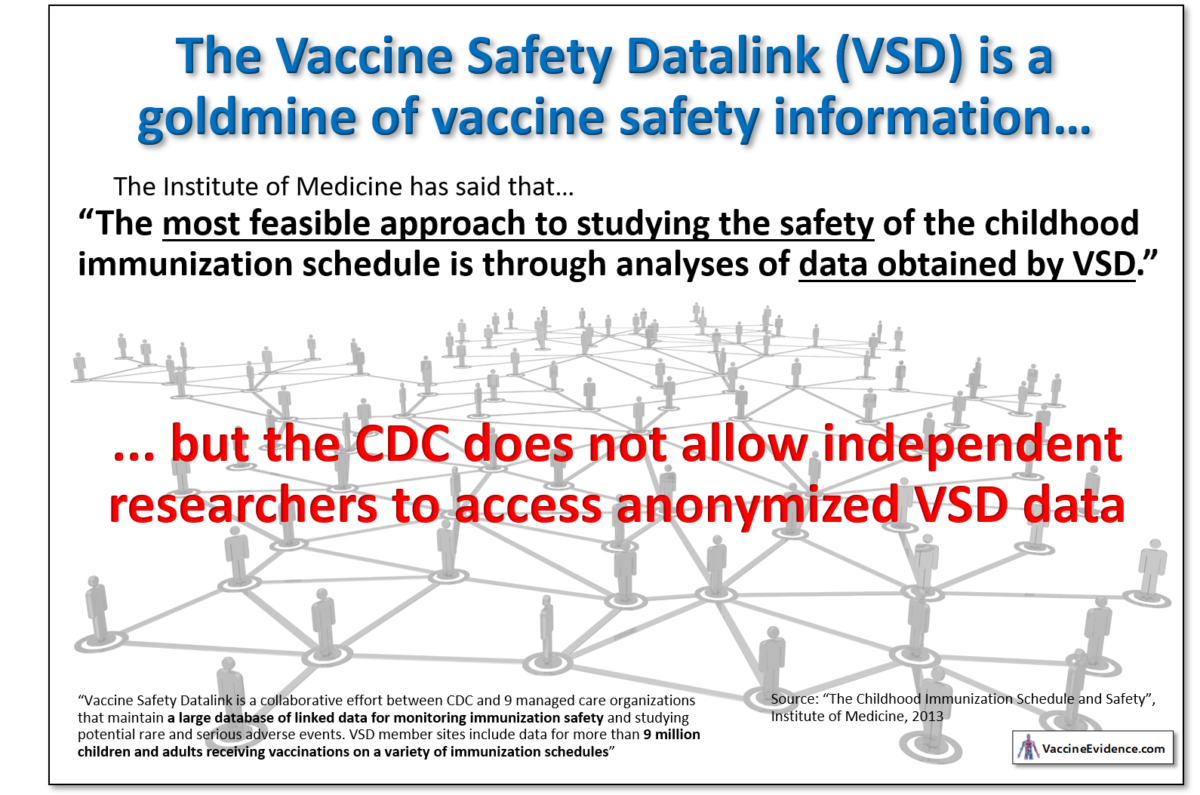
The post-approval monitoring systems of the CDC are the Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD). VAERS is a system is for reporting immediate and short-term vaccine reactions. It cannot be used to monitor, for example, whether ACVs are causing autism. The VSD is a database that could easily and cheaply be used to conduct large-scale epidemiological studies. It is a data goldmine.
The Institute of Medicine, in their 2013 report “The Childhood Immunization Schedule and Safety: Stakeholder Concerns, Scientific Evidence, and Future Studies” recommended using the VSD to assess vaccine safety:
The most feasible approach to studying the safety of the childhood immunization schedule is through analyses of data obtained by VSD. VSD is a collaborative effort between CDC and 9 managed care organizations that maintain a large database of linked data for monitoring immunization safety and studying potential rare and serious adverse events. VSD member sites include data for more than 9 million children and adults receiving vaccinations on a variety of immunization schedules.
No studies have been on VSD data looking for a possible association between ACVs and neurodevelopmental conditions. The IOM’s call for more safety studies of the vaccine schedule has gone unheeded, so far.
The VSD has great potential to increase vaccine take-up by allaying many concerns people about vaccine safety. For reasons unknown, the CDC refuses to allow researchers to access the VSD data to perform these kinds of studies. Nor has it produced any studies of its own using the VSD.
Aluminum Adjuvants used in Vaccines
The CDC provides a table showing which vaccines use aluminum-based adjuvants, other adjuvants, or no adjuvant.
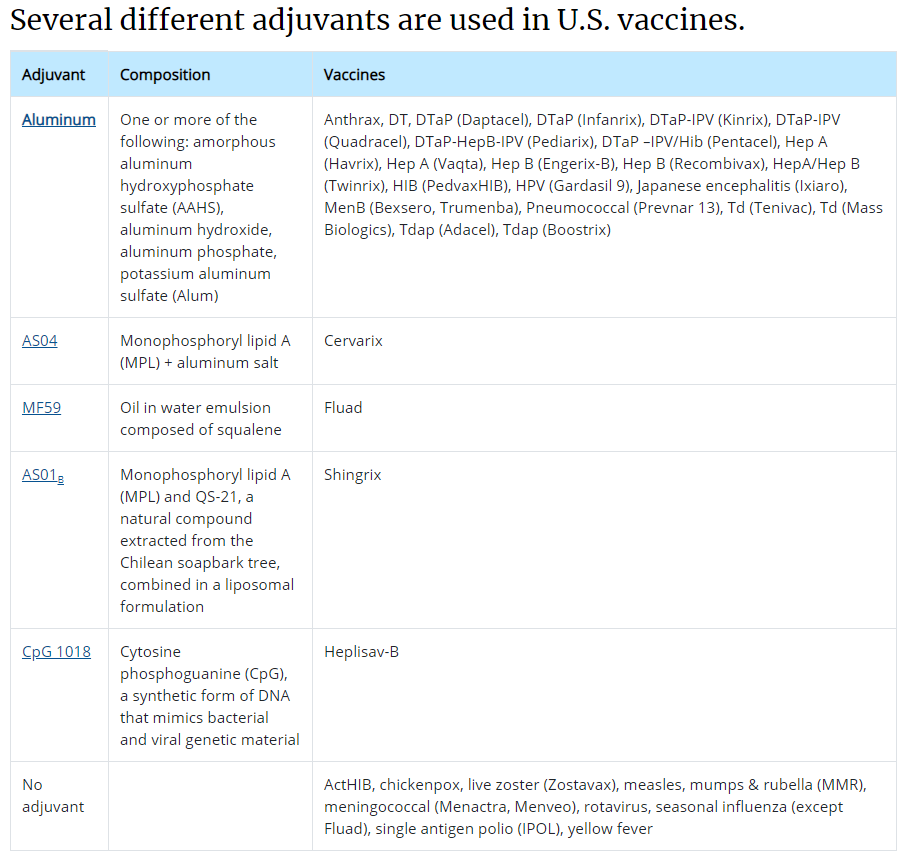
Four different aluminum salt forms are listed in the table: AAHS, AH, AP and Alum. Three of these are in vaccines on the CDC’s infant vaccination schedule.
Aluminum Salts in Infant Vaccines
The following table shows the ACVs on the CDC’s infant vaccine schedule, with the most popular brands chosen where applicable. The aluminum-weight in each dose is given, along with the aluminum salt form they use, and the ages at which doses are given.
| Vaccine | Brand | Al Content (mcg) | Adjuvant Form | Doses Given At (months) |
| HepB | Engerix-B | 250 | Aluminum Hydroxide | 0,2,6 |
| DTaP | Infanrix | 625 | Aluminum Hydroxide | 2,4,6 |
| Hib | PedvaxHIB | 225 | AAHS | 2,4,12 |
| PCV13 | Prevnar 13 | 125 | Aluminum Phosphate | 2,4,6,12 |
| HepA | Havrix | 500 | Aluminum Hydroxide | 12 |
The highest single day exposure is at 2 months old, when 1,225 mcg is injected at once. The total aluminum content of the vaccines given to infants in the first six months is 3,450 mcg (3.45 mg).
Is this a “small” amount?
The CDC writes that:
Aluminum-containing adjuvants are vaccine ingredients that have been used in vaccines since the 1930s. Small amounts of aluminum are added to help the body build stronger immunity against the germ in the vaccine.
The term “small” requires some reference value. Is 3.45 mg in six months a “small” or “large” amount of exposure to aluminum for an infant?
One way to answer this question is to compare it to aluminum exposure from other sources.
Aluminum from Vaccines vs Other Sources
The CDC writes that:
Aluminum is one of the most common metals found in nature and is present in air, food, and water.
We are indeed all exposed to aluminum in our food, drinking water, and air. By knowing the aluminum content of our food, drinking water, and air, we can estimate our total intake. Using estimates of gut and lung bioavailability, we can calculate our total uptake, i.e. how much aluminum is entering our blood.
The infographic below shows this calculation:
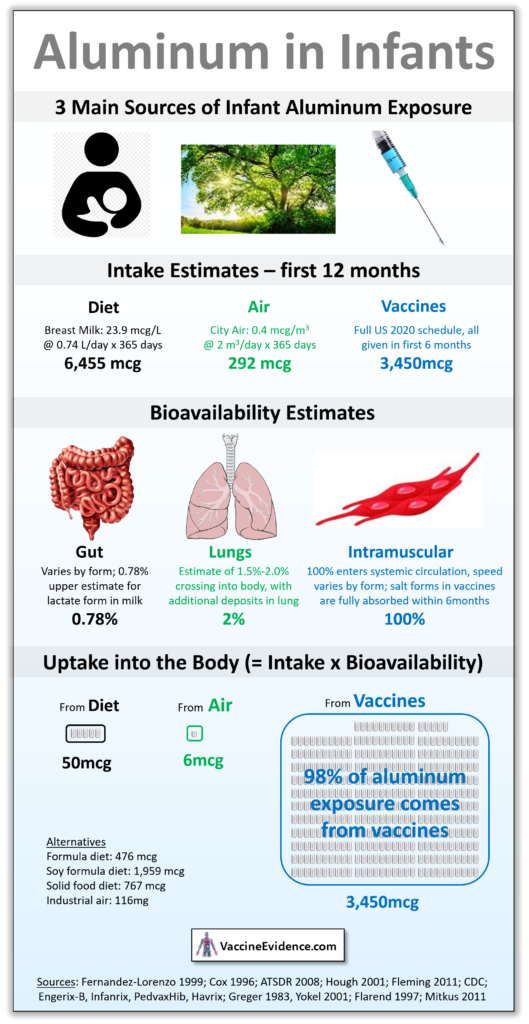
The details of this calculation and sources can be found in my post: Aluminum Uptake in Infants
It can be seen that for some infants, 98% of aluminum exposure over the year comes from their vaccines. If they are exclusively breastfed they will only uptake 50 mcg through their gut over the entire year. Exposure from city air of average quality is only 6 mcg. Even infants fed high-aluminum soy formula or grain-based baby foods will uptake no more than 2,000 mcg of aluminum through their gut. Still a lot less than the 3,450 mcg aluminum they received from their vaccines.
Since vaccines are the primary source of aluminum exposure to infants, it cannot be claimed that the amount of aluminum in vaccines is “small”.
Absorption from Vaccines
The CDC writes that:
Scientific research has shown the amount of aluminum exposure in people who follow the recommended vaccine schedule is low and is not readily absorbed by the body.
The phrase “not readily absorbed by the body” is certainly true in the case of aluminum exposure in food, drinking water, and air. Gut bioavailability (the percentage of intake that enters the blood) is less than 0.3% and lung bioavailability is only 2.0%. Hardly any of the intake from diet and air enters the body; aluminum is not readily absorbed through the guts or lungs.
Vaccines are injected into muscle. There is no way for the aluminum in vaccines to leave the injection site except by entering the systemic circulation. Thus, intramuscular bioavailability of aluminum is necessarily 100%. It is all absorbed by the body, sooner or later.
By “not readily”, the CDC means that it is absorbed slowly. There have been two studies looking at the rate of aluminum absorption from ACVs: Flarend 1997 and Weisser 2019. Both tested both aluminum hydroxide (AH) and aluminum phosphate (AP) injected intramuscularly in animals. They measured blood concentration to estimate the speed of aluminum absorption.
At the rates observed by Flarend, assuming zero-order absorption, AP vaccines take 56 days to be fully absorbed and AH vaccines take 165 days. At the rates observed by Weisser, AP vaccines take 94 days to be fully absorbed and AH vaccines take 369 days. Based on the absorption rates observed by Flarend, all aluminum from infant ACVs is fully absorbed by one year of age.
Daily Aluminum Uptake in Infancy
Is uptake of aluminum from vaccines “low” because of the slow absorption?
We can use the results of Flarend on vaccine absorption to calculate daily aluminum uptake from vaccines throughout infancy. In the chart below, daily uptake of aluminum from vaccines is plotted against uptake from diet and air. The input scenario is full vaccination on the CDC schedule, typical formula-feeding and average urban air quality.
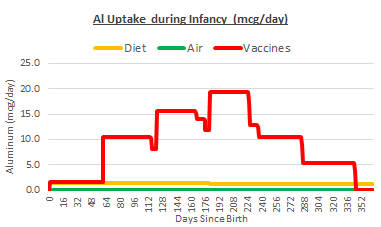
The slow absorption of the aluminum in vaccines does not alter the fact that vaccines are the biggest source of aluminum exposure in infants. At the peak, just after the 6 month shots, infants are exposed to nearly 20 mcg per day. This is the amount entering their bloodstream from each of their vaccine injection sites, like a nicotine patch. Most infants will never be exposed to more than 2 mcg per day from diet and air.
Since vaccines are the primary source of aluminum exposure to infants, it cannot be claimed that the amount of aluminum exposure is “low”.
Uptake from Vaccines v Safety Levels
Perhaps “low” is meant as compared to a safety level. Unfortunately, there are no uptake safety levels for chronic exposure to aluminum.
There are safety levels for oral intake. These have been derived from observations in animal experiments. They are the highest dose of aluminum for which no adverse effects were observed, converted to a Human-Equivalent Dose (HED). The US ATSDR set an oral intake Minimal Risk Level (MRL) of 1 mg/kgbw/day. The WHO JECFA set an oral intake safety level of 0.3 mg/kgbw/day.
These oral intake safety levels can be converted into a uptake safety levels by multiplying them by an assumed gut bioavailability of 0.3%. The units of mcg/kgbw can be converted into mcg using CDC average infant weight charts. The two derived uptake safety levels can then be added to our daily uptake chart:
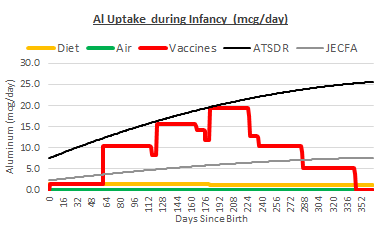
Uptake from vaccines alone far exceeds the safety level from the JECFA, and gets very close to the safety level from ATSDR. The cumulative impact of vaccines, diet, and air does exceed the ATSDR safety level for most infants. This is especially true of underweight infants and those on a high-aluminum diet.
The Mitkus Paper – The CDC’s Only Defense
The CDC ends it’s paragraph of information about aluminum adjuvant safety with this:
Read the research on aluminum exposure and vaccines. Also, see FDA’s web page on common ingredients in U.S. licensed vaccines for more information.
The first link is to a 2011 paper by Robert Mitkus and four of his colleagues at the US FDA. The paper describes a pharmacokinetic model developed for assessing the safety of ACVs in infants. The second link is to a webpage of the FDA, which refers only to the same Mitkus 2011 paper.
The CDC claims that aluminum adjuvant use is safe. Since Mitkus 2011 is the only scientific paper cited by the CDC in regard to aluminum in vaccines, this is presumably the strongest paper they can cite to support their claim. If this paper is shown to have serious flaws, it would be a crippling blow to the scientific case for vaccine adjuvant safety.
I have studied the Mitkus paper in great depth, along with the papers cited therein. I have reconstructed his whole model. I have expanded it to be able to cover more scenarios, i.e. variations in diet, air quality, vaccine schedules, etc. By doing that, I have identified many weaknesses, faulty assumptions, and outright errors.
I will explain the many flaws in the Mitkus model in future posts. In the meantime, here is an infographic explaining the most outrageous error. Mitkus used the wrong retention equation in his model!
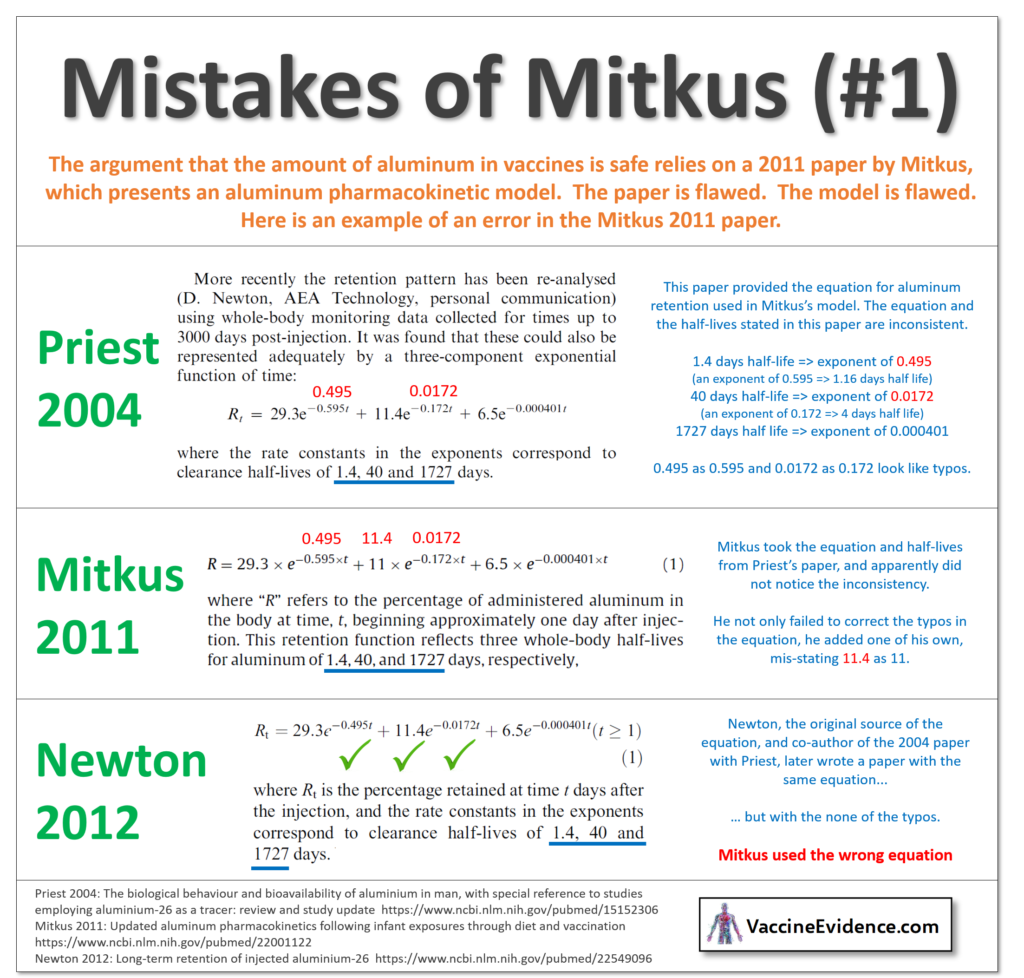
The only scientific paper cited by the CDC in defense of their claim that aluminum adjuvants are safe contains this outrageous error, and there are many more.
Conclusion
There are good reasons to be concerned about aluminum adjuvant safety. Aluminum is a neurotoxin that can subtly alter neurodevelopment. It’s use in vaccines has increased over the years, in line with the increase in neurodevelopmental disorders.
The CDC is incorrect in describing the amount of aluminum in vaccines as “small” or total exposure from vaccines as “low”. Vaccines are in fact the primary source of aluminum exposure in infants. The CDC should update their website to remove these inaccurate descriptions.
Aluminum exposure from the vaccines on the CDC’s infant schedule exceeds the safety level established by the WHO. This calls for a reappraisal of the vaccine schedule: delaying or avoiding ACVs to reduce the risk of adverse neurodevelopmental effects from vaccines.
The CDC’s claim that aluminum exposure from vaccines is low enough to be considered safe relies on one single paper: a deeply flawed study by the FDA, presenting a pharmacokinetic model with many serious errors.