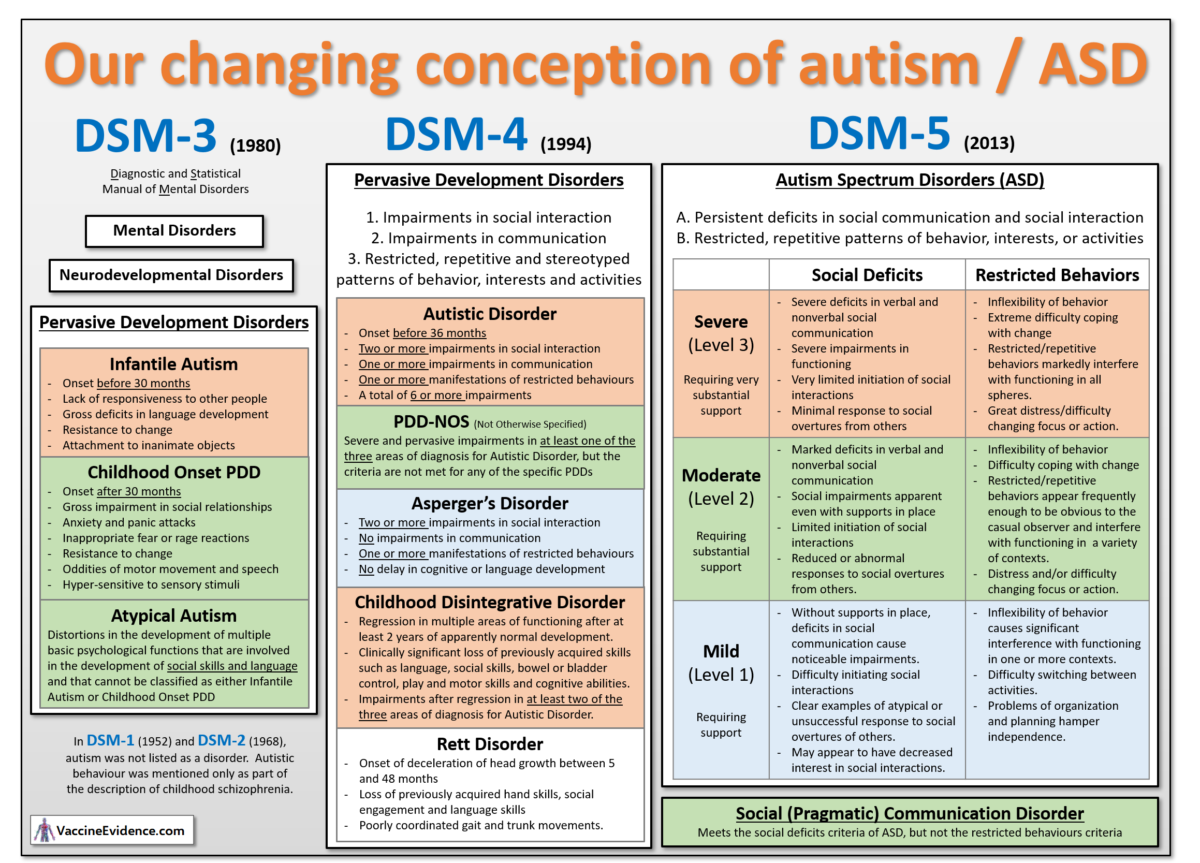
Our understanding and conception of autism has changed considerably over the years, as shown in the infographic above.
Autism Before 1980
The first recognition of autism only occurred in 1943, and for decades it was believed to be very rare, affecting only 1-in-10,000 children. The first time the American Psychiatric Association (APA) published their list of all known mental disorders, the prestigious Diagnostic and Statistical Manual of Mental Disorders or DSM-1 (1952), it did not include autism. It used the word autistic only in reference to one of the behaviours associated with childhood-onset schizophrenia. Autism was also not listed in the second edition, DSM-2 (1968).
Autism in DSM-3
Autism was first listed as a known mental disorder in DSM-3 in 1980. A category of neurodevelopmental (early onset) disorders was created called the Pervasive Development Disorders (PDDs), which contained infantile autism for when autistic behaviours appeared before 30 months of age and childhood onset PDD for when they appear after 30 months of age.
These autistic behaviors include lack of responsiveness to other people, deficits in language development and social relationships, resistance to change, attachment to inanimate objects, anxiety and panic attacks, inappropriate fear or rage reactions, oddities of motor movement, and speech and hyper-sensitivity to sensory stimulation.
A third PDD was atypical autism, a catch-all for when there were impairments in social skills and language but the criteria for a specific PDD cannot be met.
Autism in DSM-4
The DSM-4 in 1994 introduced three areas of diagnosis for the PDDs: impairments in social interaction, impairments in communication, and restricted, repetitive and stereotyped patterns of behavior, interests and activities. It also renamed and reformulated the PDDs.
Autistic Disorder required onset before 36 months of age and at least 6 of the 12 impairments listed across the three areas of diagnosis. Those previously diagnosed with infantile autism would in the new system likely be diagnosed with autistic disorder. Those previously diagnosed with childhood onset PDD or atypical autism would likely be diagnosed with PDD-NOS (for Not Otherwise Specified), the new catch-all for where there are severe deficits in one of the three areas of diagnosis but the criteria are not met for any of the specific PDDs.
Three new PDDs were added: Asperger’s Disorder was created for those with impairments in social interaction and restricted behaviours, but no impairments in communication, cognition or language skills, and it was considered “mild autism” or “high-functioning autism”. The other two new additions were Childhood Disintegrative Disorder (CDD), a sudden and severe regressive disorder in multiple areas of functioning with subsequent onset of autistic behaviors, and Rett’s Disorder, a regressive disorder affecting head growth, motor skills, gait and trunk movements, as well as autistic behaviours. These are both very rare disorders, and Rett’s Disorder is now considered a genetic brain disorder rather than an autism spectrum disorder or PDD.
Asperger’s makes up 17% of cases of PDD, autistic disorder is 31%, but the largest group is PDD-NOS at 53% (Hviid, 2019). The addition of Asperger’s Disorder (and to a much lesser extent, CDD and Rett’s) would thus have caused only a small step change – ceteris paribus – in the number of people diagnosed with a PDD, as DSM-4 replaced DSM-3.
Autism in DSM-5
The DSM-5 in 2013 replaced the PDD category entirely and replaced it with Autism Spectrum Disorder (ASD). The PDDs were already considered a spectrum widely known as the autism spectrum, ranging from the most severe (Autistic Disorder) to the less severe (PDD-NOS and Asperger’s). Autism was no longer the name of one type of PDD, but the whole category, and it was defined as a single spectrum disorder rather than a category of related disorders with distinct names, as PDD had been.
Within ASD, there is a classification by severity in two dimensions: 1) deficits in social interaction and communication, and 2) restricted, repetitive behavior, interests, or activities. Three severity levels (mild, moderate and severe) are defined by how much support the individual requires. Most of those previously diagnosed with autistic disorder would now be diagnosed with moderate or severe ASD (aka autism), while most of those previously diagnosed with Asperger’s disorder would now be diagnosed with mild or moderate autism. It is possible to be diagnosed as having one severity level for social deficits and a different severity level for restricted behaviors, giving nine possible severity level combinations within the spectrum.
The DSM-5 also created a new neurodevelopmental disorder called Social (Pragmatic) Communication Disorder (SCD) for cases that meet the social deficits criteria for ASD but not the restricted behaviors criteria. According to one study (Kim, 2014), only 63% of those with a previous diagnosis of PDD-NOS meet the DSM-5 criteria for ASD, with 32% lacking the restrictive behaviours criteria and so would now be diagnosed with SCD, not ASD. Those previously diagnosed with PDD-NOS who do meet the ASD criteria are likely to have either a mild or moderate DSM-5 severity level (Walker, 2004).
The impact of a third of those with PDD-NOS (the largest PDD disorder) being taken out of the umbrella of ASD should have a noticeable decrease – ceteris paribus – in autism diagnoses as DSM-5 replaces DSM-4. The definition of ASD in DSM-5 is tighter than the definition of PDD in DSM-4 and may be tighter than the definition of PDD in DSM-3 as well.
Autism in ICD-10 Codes
The World Health Organisation (WHO) maintains a comprehensive medical coding system known as the International Classification of Diseases (ICD). The current iteration of this system is ICD-10, which has been used since 1994. Chapter 5 contains the codes for mental and behavioural disorders (F00-F99) and it has codes for “childhood autism” (F84.0), “atypical autism” (F84.1) and Asperger’s disorder (F84.5), “Other PDD” (F84.8) and “Unspecified PDD” (F84.9) all within the category of pervasive development disorders (F84).
These five ICD-10 codes are considered to cover the whole autism spectrum and epidemiological studies of autism generally define an outcome of autism as a diagnosis with one of these five ICD-10 codes (for example, Hviid 2019).
These codes map easily to the disorders in DSM-4 and DSM-3: childhood autism is the same as infantile autism (DSM-3) and autistic disorder (DSM-4); Asperger’s Disorder is defined the same way as in DSM-4; PDD-NOS (DSM-4) is split between ICD codes for atypical autism, other PDD and unspecified PDD, with atypical autism being defined in a way similar to the DSM-3 definition.
Autism Diagnostic Criteria
Despite the many taxonomical changes within the PDD / ASD category of disorders over the years, the diagnostic criteria have been refined and elaborated with each iteration of the DSM, but the basic idea has always been the same. Autism has always been defined as a disorder with two fundamental defining elements: deficits in social communication and social interaction, and restricted, repetitive patterns of behavior, interests and activities.
DSM-5 gives the clearest diagnostic criteria for each of these two elements. It provides three illustrative examples of social deficits, all of which must be met for a diagnosis, and four illustrative examples of restricted behaviors, two of which must be met for a diagnosis. The examples are:
Persistent deficits in social communication and social interaction across multiple contexts, as manifested by ALL OF the following, currently or by history:
- Deficits in social-emotional reciprocity, ranging, for example, from abnormal social approach and failure of normal back-and-forth conversation; to reduced sharing of interests, emotions, or affect; to failure to initiate or respond to social interactions.
- Deficits in nonverbal communicative behaviors used for social interaction, ranging, for example, from poorly integrated verbal and nonverbal communication; to abnormalities in eye contact and body language or deficits in understanding and use of gestures: to a total lack of facial expressions and nonverbal communication.
- Deficits in developing, maintaining, and understanding relationships, ranging, for example, from difficulties adjusting behavior to suit various social contexts; to difficulties in sharing imaginative play or in making friends; to absence of interest in peers.
Restricted, repetitive patterns of behavior, interests, or activities as manifested by AT LEAST TWO of the following, currently or by history:
- Stereotyped or repetitive motor movements, use of objects, or speech (e.g., simple motor stereotypies, lining up toys or flipping objects, echolalia, idiosyncratic phrases).
- Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, need to take same route or eat same food every day).
- Highly restricted, fixated interests that are abnormal in intensity or focus (e.g., strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interests).
- Hyper- or hyporeactivity to sensory input or unusual interest in sensory aspects of the environment (e.g., apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement).
For a diagnosis of ASD, symptoms must also be present in the early developmental period (but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life), they must cause clinically significant impairment in social, occupational, or other important areas of current functioning, and these disturbances are not better explained by intellectual disability or global developmental delay.
Clinical Significance
The requirement for onset during the “early developmental period,” meaning early childhood, obviously means that adults cannot develop autism. However, adults can be and are diagnosed with autism if they are impaired significantly enough by their social deficits and repetitive behaviors today to warrant a diagnosis, without any evidence that their autistic behavior started in the early developmental period. The age of onset diagnosis criteria is essentially ignored as it is assumed that any adult that meets the criteria for autism today must have been autistic their whole life.
The requirement for “clinically significant impairment” is standard wording throughout the DSM-5 for all mental disorders. It means that it is left entirely at the discretion of clinicians to judge whether a child (or adult) is impaired *significantly enough* by his social deficits and repetitive behaviors to get a diagnosis of ASD. Clinicians get to draw the line between marginal cases of mild ASD and no ASD, and where they draw that line is flexible and may have changed over time to include more people: an adult previously considered merely as having autistic-like traits (perhaps an introvert with restricted interests, a geek or an eccentric) may now get a diagnosis of ASD, if he seeks one. There are incentives for adults to get a diagnosis, for parents and schools to have their children diagnosed, and for clinicians to give diagnoses in marginal cases. There is a clear danger of over-diagnosis of autism due to the flexibility of the clinical significance requirement, and this must be borne in mind when looking at historical statistics of autism prevalence and incidence.
Conclusion
Clear and well-understood definitions are essential for productive discussion and good science. When discussing autism, it is important that all the participants understand whether the term is being used:
- in the wider sense of anyone on the autism spectrum in the DSM-5 conception, roughly equivalent to what DSM-4 called PDDs
- in the narrower sense of autistic disorder (only 31% of PDDs) in the DSM-4 conception, roughly equivalent to severe autism in the DSM-5 conception.
The wider sense includes those with Asperger’s (17%) and PDD-NOS (53%), which are likely mild or moderate autism in the DSM-5 conception.
When discussing autism, when reviewing data from epidemiological studies, comorbidity studies, historical trends, independence surveys, and so on, it is crucial to understand if the data refers to the whole autism spectrum or just those with severe autism, or those with autism and some other condition comorbid with autism, such as a language disorder or intellectual disability.